

According to a 2011 Institute of Medicine of the National Academies report entitled “Relieving Pain in America_” an estimated 100 million Americans alone suffer from some form of chronic pain. A significant percentage of that pain, estimated to be around 9%, falls into the category of “shoulder pain that has lasted for at least three months“. Specific causes range from serious traumatic injury, to simple overuse and overstretching of muscles and tendons. (Not surprisingly, athletes and manual workers are disproportionately affected by chronic shoulder pain.) The current analysis is geared toward the latter, as opposed to the former cause of shoulder pain, where consultation with an orthopedic specialist is perhaps warranted.
To begin with, the human shoulder is nothing less than an evolutionary miracle which allows us to flexibly position our arms for full use in performing tasks associated with sport, work, or simple everyday activities. Let’s start with a brief review of the muscles that make up the shoulder, which can often be the source of chronic shoulder pain:
Principal shoulder muscles
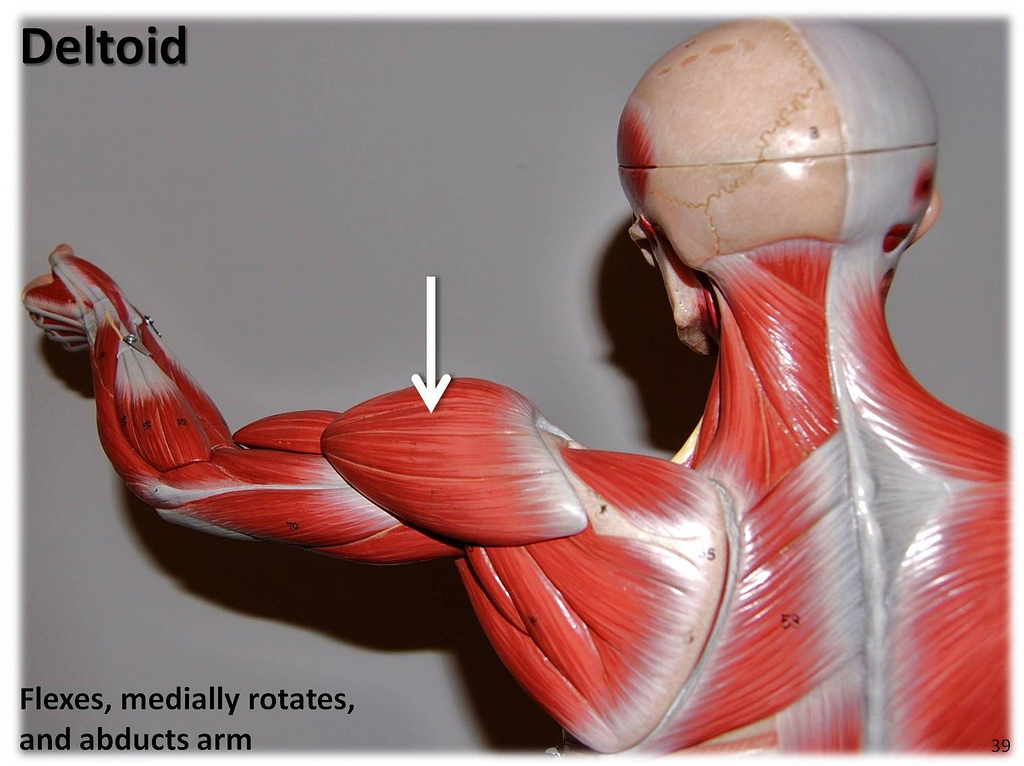
The big muscle that forms the rounded contour of your shoulder is named the deltoid muscle. This is a muscle often targeted by body builders, and one which is easily strained by strenuous activities such as weight lifting or performing pushup exercises. It is an exceptionally strong muscle, because it has to prevent dislocation of the large bone in the upper arm called humerus. We illustrate below:
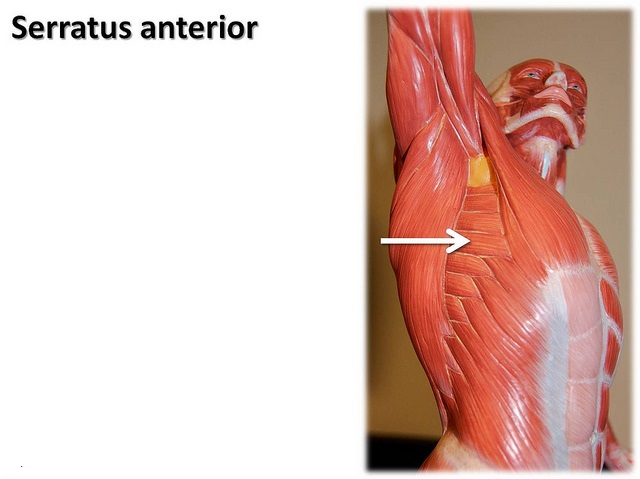
The long thin muscle running under the “armpit” called serratus anterior, although not technically part of the shoulder, often is involved in shoulder pain. For this reason it is also illustrated:
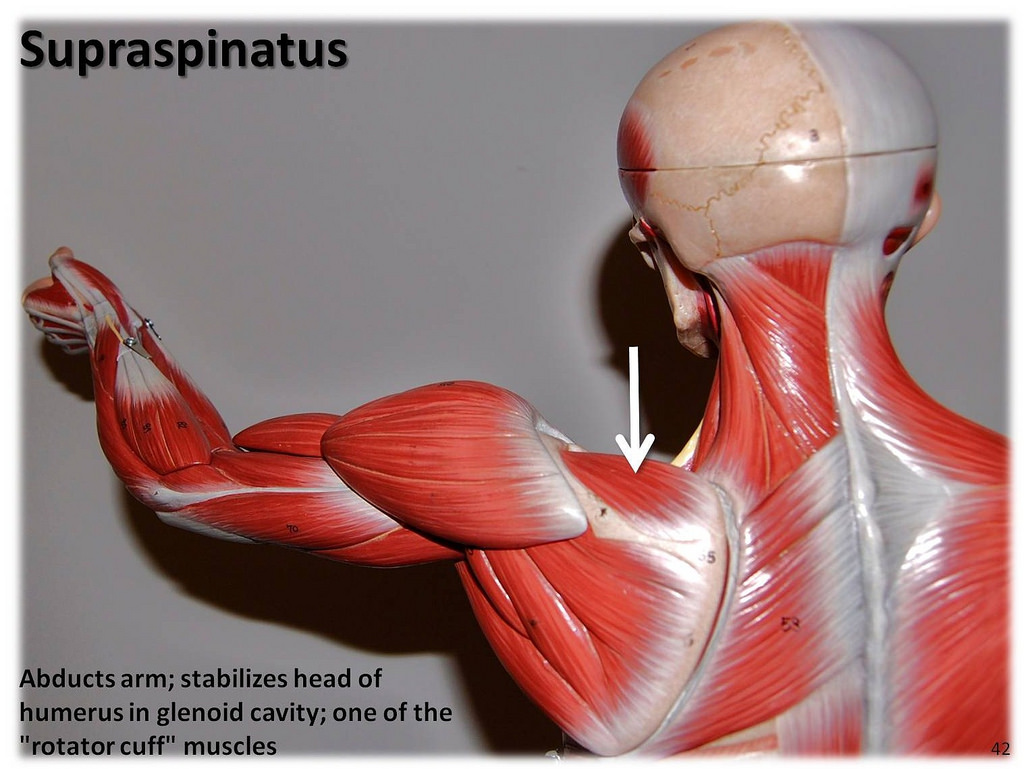
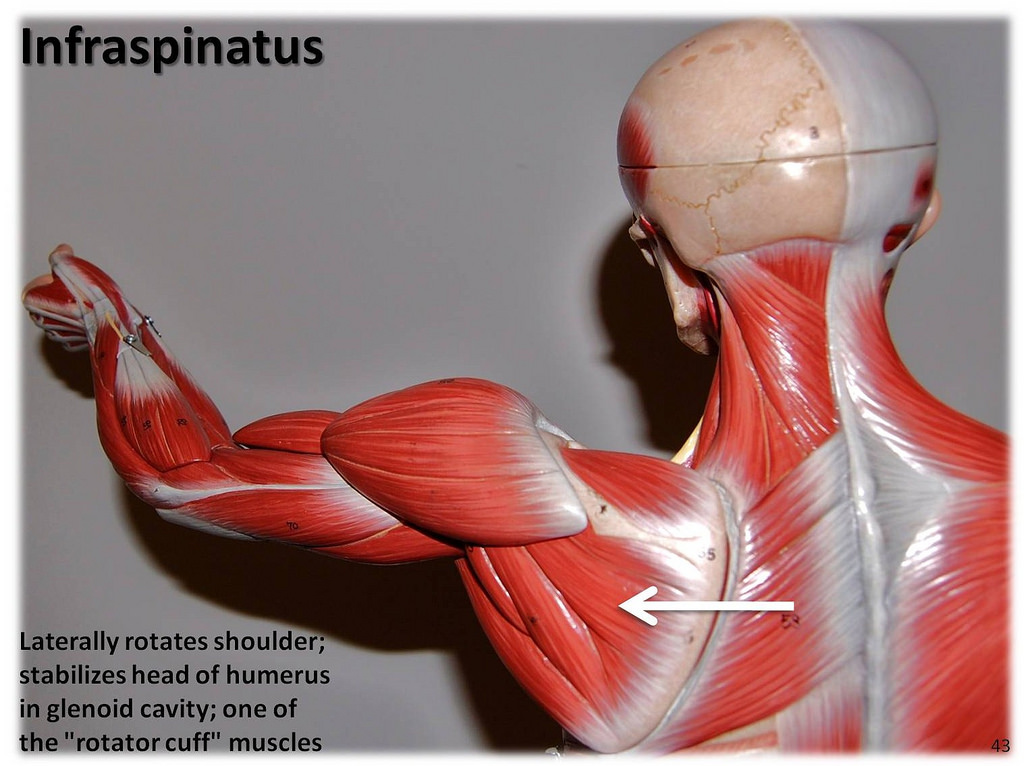
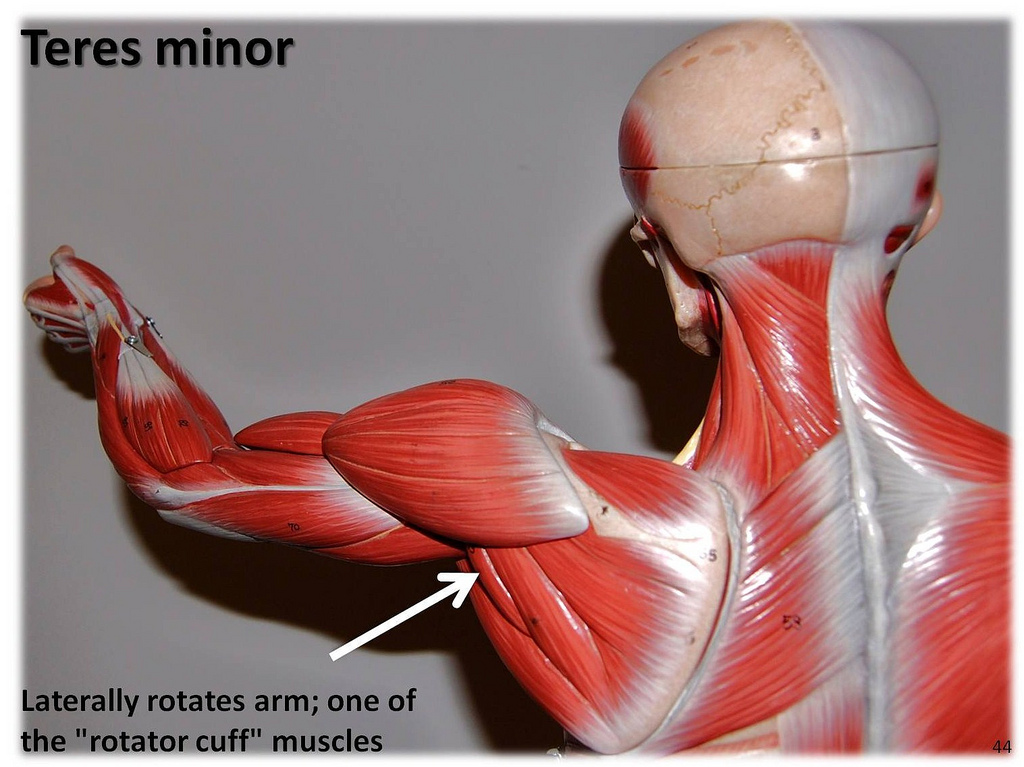
The group of muscles referred to as rotator cuff plays an important role in both shoulder movement, and in maintaining joint stability. These muscles are involved in arm abduction (pulling arms away from body) and also allow us to rotate our shoulders both internally and externally. Primary rotator cuff muscles are supraspinatus, infraspinatus, teres minor, and subscapularis. Each is also illustrated below, with the exception of subscapularis which, as the name implies, is a deeply embedded muscle:
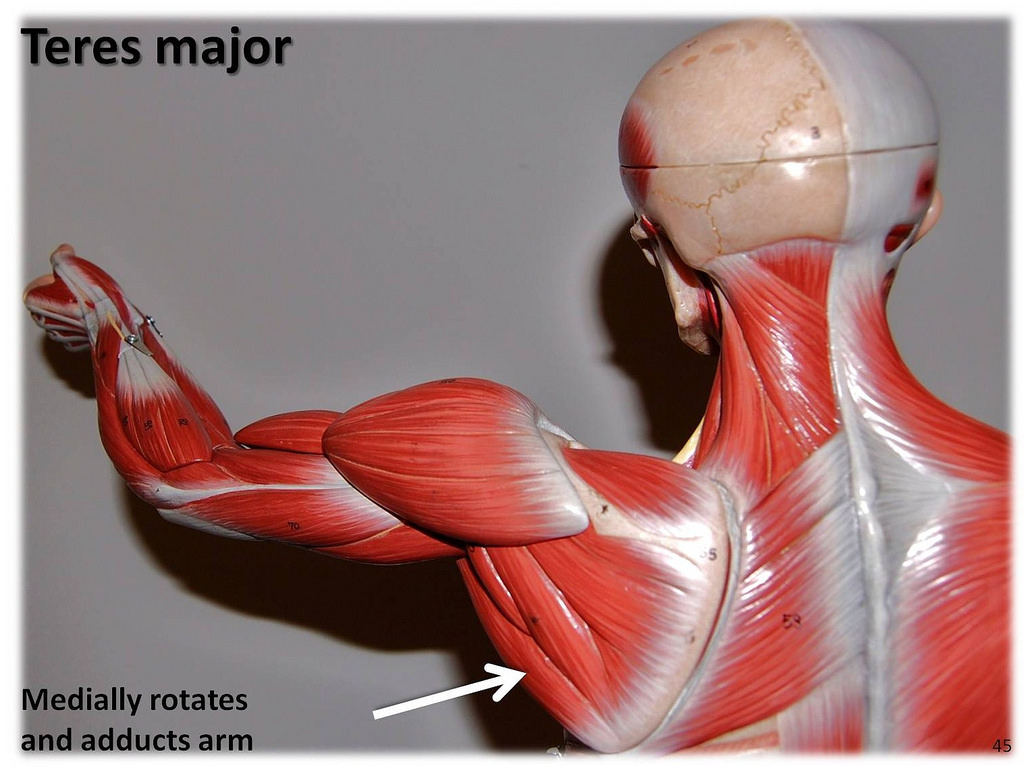
Finally, there’s teres major which is located directly below teres minor:
In addition, each rotator cuff muscle has tendons associated with it which are also susceptible to strain injury. Tendons are composed of fibrous connective tissue which connect muscle to bone.
Conventional responses to shoulder pain
Those of us who are physically active are aware of the standard recommended immediate treatment for any muscle or tendon strain: R.I.C.E, an acronym for rest, ice, compression, and elevation. The details of R.I.C.E. may be found on most popular websites such as webmd.com, so that I will not bore you by repeating them here. After a few days have passed, stretching exercises and the application of heat is recommended. (see, for example,U.S. National Library of Medicine-Medline plus at nlm.nih.gov/medlineplus) For chronic shoulder pain that lasts more than a few weeks, local anesthetic injections may be used alone, or in conjunction with physical therapy. This may be followed by corticosteroid injections and surgery. Steroid side effects include osteoporosis and aseptic necrosis or “bone death”. Prescription pain killers are also frequently prescribed which provide symptomatic relief only. Unfortunately, addiction to these medications is becoming a national health crisis. (see “Drugs of Abuse: Opioids; National Institute of Drug Abuse, 2015).
It is no wonder that more and more chronic shoulder pain sufferers are seeking alternative “natural” cures. In our current segment, Spanking FIT examines a few of them from a scientific legitimacy perspective.
Proposed “natural” chronic shoulder pain remedies:

Myofascial trigger point therapy (M.T.P.T.)
In 1983, Janet Travell, M.D., a one-time personal physician to President J. Kennedy, first published Myofascial Pain and Dysfunction- The Trigger Point Manual. In it she presented the modern theory of myofascial trigger point therapy. (I underscored modern, because this theory bears a certain resemblance to centuries-old forms of oriental medicine, so that it may not be entirely original.)
To understand M.T.P.T., one should begin by knowing that our skeletal muscles do not exist freely, but are separated and surrounded by bands of fibrous connective tissue made of collagen that are called fascia. These fascia are supplied with sensory nerve receptors that make them a potential source of chronic pain. According to M.T.P. T. theory, small nodules or knots referred to as “trigger points“can develop in fascia as a result of injury or excessive muscle strain. Trigger points may cause further damage by cutting off blood supply to the immediate area where located. Advocates of M.T.P.T. believe it is possible to relieve pain through elimination of “taut muscle bands” containing trigger points using massage and other related manipulative methods.
Before examining the scientific evidence behind these claims, I should remark that M.T.P. therapy is still highly controversial within the so-called conventional medical community. For example, in “A critical evaluation of the trigger point phenomenon” by John Quintner, M.D. et al., published in Rheumatology, 2015; 54(3), opinion is given that M.T.P. therapy is “an invention that has no scientific basis” and that the theory is “flawed both in reasoning and in science”. Dr. Quintin is an internationally recognized “specialist” in rheumatology and “pain medicine”.
Research supporting M.T.P. T. efficacy
Among most detailed scientific studies from a statistical design perspective is: “Treatment of myofascial trigger points in patients with chronic shoulder pain _” by Carel Bron, et al. published in B.M.C. Medicine, Jan. 2011. Interestingly, Dr. Quintner and his associates above overlooked it in their previously cited critique. The Bron study was a randomized controlled trial (r.c.t.) as opposed to the more common observational kind; and, therefore offers better potential to yield credible findings. It was also particularly relevant in so far as it dealt specifically with the topic of shoulder pain. In their experiment, 65 chronic shoulder pain patients were randomly assigned to either a treatment or a control group. A number of outcome measurements were employed for comparison purposes including one based on a Disabilities of Arm, Shoulder, and Hand (D.A.S.H.) questionnaire. Treatment consisted mainly of M.T.P. therapy. Controls on the other hand undertook pain “self-management” and “medication at their own discretion”. After 12 weeks, outcome measures for treatments were compared with controls. The reported findings included a statistically significantly higher proportion of patients in the treatment group who exhibited a “minimally clinically important difference” (M.C.I.D.) (44% versus 23%, for treatments versus controls ) In other words, a greater proportion of M.T.P.T. treated patients exhibited substantial improvement. Furthermore, researchers reported that the mean number of muscles with “active” myofascial trigger points after twelve weeks of therapy was significantly lowered in the treated group, also indicating a strong correlation between shoulder pain and the presence of these fascia trigger points. (Sample sizes used were large enough for legitimate statistical inferences to be made.)
However, this study contains several weaknesses from a design perspective: first, a placebo was not employed in the control group. It would have been better to have used a “sham” therapy in the control group, so that the objection that the treated group experienced a placebo effect could be overcome. (You will recall that a placebo effect occurs when persons who believe they are being treated report improvement due to psychological factors only.) More importantly, upon careful examination of treatment protocols, Spanking FIT noted that the administered treatment consisted of a bit more than M.T.P.T. – it included prescribed home stretching and relaxation exercises with application of heat, also. Consequently, the objection may be raised that the observed improvements in treatment group were confounded by the effects of additional therapy interventions not included in control group. Nice try, anyway, on the part of these researchers.
One of Bron’s referenced studies is:”Chronic shoulder pain of myofascial origin: an r.c.t. using ischemic compression therapy” by G. Hains published in Journal of Manipulative Physio Therapy, June 2010. In this r.c.t., 59 patients who reported experiencing shoulder pain on a daily basis for the previous three months were randomly assigned to a treatment or a sham therapy group. The treatment consisted of M.T.P.T. sessions three times per week for five weeks. The sham therapy consisted of M.T.P.T. on trigger points located in irrelevant muscles of the cervical and upper dorsal regions of the body. Outcome comparisons were made including a Shoulder Pain and Disability Index (S.P.A.D.I.) questionnaire. Using repeated measures A.N.O.V.A. methods, researchers reported a statistically significant improvement in the actual therapy group, versus the sham therapy. Furthermore, this perceived improvement was reported to have lasted up to six months following therapy. Patients in the control group that subsequently underwent M.T.P.T., also showed significant improvement.
One drawback to this study, which the authors themselves acknowledge, was the small sample size of only 18 patients in the control group. Nevertheless, this study lends some credibility to the M.T.P.T. efficacy hypothesis, in my opinion.
Finally, Spanking FIT came upon “Effects of traditional Thai self-massage using a Wilai massage stick (T.M.) versus ibuprofen in patients with upper back pain associated with myofascial trigger points” by P. Wamontree and published in Journal of Physical Therapy Science, Nov. 2015. In it, 65 patients diagnosed with upper back pain were randomly assigned to either self massage with a Wilai stick, or to ibuprofen for five days. Both groups were advised to perform identical stretching exercises and given detailed massage instructions. Using the statistical technique of repeated measures A.N.C.O.V.A., researchers reported significant improvements in all measured outcomes for the treatment group including a decrease in perceived intensity of pain, increase in pressure pain thresholds, and decreased tissue hardness. In the control group, only the perceived intensity of pain decreased significantly as would be expected with ibuprofen use. Just as importantly, there were reported significant differences between treatment versus controls, with the M.T. P. -treated patients performing better than the ibuprofen-treated on all outcome measures.
I was disappointed , however, to detect a hint of a conflict of interest on the part of the authors. Their study was funded in part by the Thai Traditional Knowledge Medicine Fund, which in turn appears to be partly funded from the licensing fees of traditional medicine practitioners. Furthermore, it was conducted at the Traditional Thai Medical Clinic of Lat Lukaew Hospital, a provider of traditional Thai medicine. This study, nevertheless, makes a good case for general M.T.P.T., assuming integrity on the part of principal investigators.
While not completely validating M.T.P.T. theory, all of the above research does lend some credibility to it. Nevertheless, millions of chronic pain sufferers each year seek help from chiropractors and other practioners who employ M.T.P. techniques. Many even employ M.T.P. self-massage to save on time and on chiropractic costs:
Soothing myofascial self-massage

An essential initial step before performing self-massage is location of the relevant shoulder muscles. The previously presented anatomy diagrams may be used for this purpose. Since theorists believe that problems in one muscle can create “referred pain” in others, they recommend massaging all shoulder muscles including deltoids and those of the rotator cuff in order to achieve maximum benefits. For muscles that can be accessed by hand such as supraspinatus, a “manual press and move technique” is often suggested. This involves pinching and pressurizing the muscle in order to cause it to move. Self-massage of hard to reach muscles may cleverly be achieved by placing a hard round object such as a tennis ball between muscle and a wall. Above is an illustration of certified M.T.P. therapist Jan Linden performing self-massage of his deltoid muscle while standing behind a glass panel. (Of course, as already mentioned, it is recommended that you use a real wall.) In performing tennis ball self-massage, Jan suggests placing the ball over the muscle and to slowly rub over it searching for either tight or tender spots. Such spots “should be massaged using approximately 10-15 strokes”. The degree to which it is effective depends on the individual. Nevertheless, it is one heck of a soothing massage! You can get further info about this at painotopia.com.
Shoulder pain and nutrition-the vitamin D connection

Proper nutrition is highly recommended for the prevention and the treatment of of all muscle strain that can lead to chronic pain. Adequate amounts of protein consumed in the diet provide the amino acids essential for rebuilding damaged tissue. Vitamins A and D in particular are believed to play an important role in healing muscle and in collagen production. Collagen is a protein commonly found in connective tissue including previously spotlighted muscle fascia. Adequate consumption of minerals such as Iron, Magnesium, Calcium, Copper, and Zinc is also essential. Minerals attach themselves to the active molecular sites of enzymes and antioxidants such as super oxide dismutase which protect muscle tissue.
Among the substances most often overlooked for its muscle-healing potential is Vitamin D. Vitamin D, in its many forms, is a secosteroid hormone long recognized for playing an important role in building human bone. However, scientific evidence is mounting that it also plays an essential role in maintaining muscle health. In “Nude Sunbathing-It Does a Body Good”, Spanking FIT, Aug. 2015, I cited research supporting claim that vitamin D supplementation, either through diet or through sunshine exposure, may safely enhance testosterone and IGF1 levels in the human body. IGF1 not only stimulates growth of cartilage and bone, but of skeletal muscle, also. What follows are the results of Spanking FIT‘s evaluation of research supporting the vitamin D/ muscle health hypothesis:
In “Ultraviolet radiation and altitude fitness” by G. Lehman published in Luftfahrmedizin in 1944, investigators irradiated 32 German medical students for six weeks and reported a 13% improvement in skeletal muscular performance as measured using a bike ergonometer. Similar findings were reported by Spellerberg in his 1952 publication: “Increase of athletic effectiveness by systematic ultraviolet radiation” published in Strahlentherapie (88). In both experiments, improvements may be attributed to increased vitamin D production. In “Low-dose vitamin D prevents muscular atrophy_” by Y. Sato and published in Cerebrovascular Disease, 2005 (3), researchers presented results of a randomized controlled trial involving vitamin D deficient elderly patients who were also, as a consequence of suffering a stroke, hemiplegic (i.e., paralyzed in half of their bodies) . 96 patients were randomly assigned to either a treatment consisting of 1,000 I.U. of ergocalciferol (vitamin D2) supplement daily, or a placebo. Researchers reported significant increases in both the relative size and the number of type II muscle fibers, as well as improvement in muscle strength in the vitamin D treated group. Type II muscle fiber is used primarily for long-term anaerobic activity. Lastly, in “The levels of vitamin D in the serum correlates with fatty degeneration of muscles of the rotator cuff” by J.H. Oh (published in The Bone and Joint Journal, Nov. 2009, 338), patients with shoulder disorders were examined and graded with respect to the degree of fatty degeneration of their rotator cuff muscles. Serum levels of D3 were measured, also. Analysis of data demonstrated a statistically significant negative correlation between the two. That is to say that patients having a greater degree of muscular degeneration also tended to have lower vitamin D levels in their blood. While not proving that vitamin D deficiency is causal for muscular degeneration or injury, the latter results suggest that vitamin D supplementation may possibly play an important role in rehabilitation.
Conclusion

Chronic shoulder pain is a major medical problem which affects millions of people including manual workers and athletes, alike. Legitimate concern about the side effects of traditional medications including osteoporosis, bone death, and addiction has led many sufferers to consider more natural alternative treatments. Options include myofascial trigger point therapy (M.T.P.T.). Spanking FIT’s thorough evaluation of relevant experimentation suggests M.T.P.T efficacy. Nevertheless, further experimentation needs to be performed for it to be completely validated, in my opinion.
Proper nutrition and dietary supplementation with minerals and vitamins, especially vitamin D, may also provide a safer alternative treatment avenue . Vitamin D, obtained either through sunshine exposure or through diet, has been recognized for a long time as playing an important role in calcification of bone. Serious experimental findings suggest that it may be just as valuable in maintaining a healthy skeletal muscular system, and in accelerating the muscle healing process. One final point: regular exercise is also extremely important in maintaining muscle health. For this I recommend reading “Healthy Body Art- Broad Shoulders” for relevant exercises. Thanks again. As usual, I look forward to receiving your valuable feedback for improving our knowledge base. Sincerely, Dr. Garrett
Featured photo credit:
https://www.flickr.com/photos/chrishunkeler/6859078957/
no changes madeCreative commons license: https://creativecommons.org/licenses/by-sa/2.0/